
This post focuses on the intake of two main plant foods, namely wheat flour and rice intake, and their relationships with mortality from all cardiovascular diseases. After many exploratory multivariate analyses, wheat flour and rice emerged as the plant foods with the strongest associations with mortality from all cardiovascular diseases. Moreover, wheat flour and rice have a strong and inverse relationship with each other, which suggests a “consumption divide”. Since the data is from China in the late 1980s, it is likely that consumption of wheat flour is even higher now. As you’ll see, this picture is alarming.
The main model and results
All of the results reported here are from analyses conducted using WarpPLS (). Below is the model with the main results of the analyses. (Click on it to enlarge. Use the "CRTL" and "+" keys to zoom in, and CRTL" and "-" to zoom out.) The arrows explore associations between variables, which are shown within ovals. The meaning of each variable is the following: SexM1F2 = sex, with 1 assigned to males and 2 to females; MVASC = mortality from all cardiovascular diseases (ages 35-69); TKCAL = total calorie intake per day; WHTFLOUR = wheat flour intake (g/day); and RICE = and rice intake (g/day).
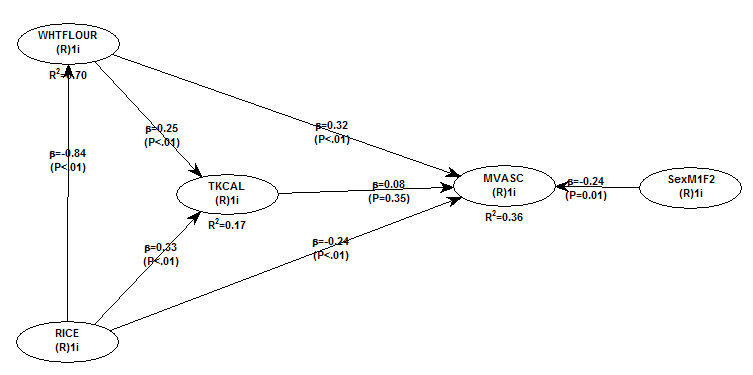
The variables to the left of MVASC are the main predictors of interest in the model. The one to the right is a control variable – SexM1F2. The path coefficients (indicated as beta coefficients) reflect the strength of the relationships. A negative beta means that the relationship is negative; i.e., an increase in a variable is associated with a decrease in the variable that it points to. The P values indicate the statistical significance of the relationship; a P lower than 0.05 generally means a significant relationship (95 percent or higher likelihood that the relationship is “real”).
In summary, the model above seems to be telling us that:
- As rice intake increases, wheat flour intake decreases significantly (beta=-0.84; P<0.01). This relationship would be the same if the arrow pointed in the opposite direction. It suggests that there is a sharp divide between rice-consuming and wheat flour-consuming regions.
- As wheat flour intake increases, mortality from all cardiovascular diseases increases significantly (beta=0.32; P<0.01). This is after controlling for the effects of rice and total calorie intake. That is, wheat flour seems to have some inherent properties that make it bad for one’s health, even if one doesn’t consume that many calories.
- As rice intake increases, mortality from all cardiovascular diseases decreases significantly (beta=-0.24; P<0.01). This is after controlling for the effects of wheat flour and total calorie intake. That is, this effect is not entirely due to rice being consumed in place of wheat flour. Still, as you’ll see later in this post, this relationship is nonlinear. Excessive rice intake does not seem to be very good for one’s health either.
- Increases in wheat flour and rice intake are significantly associated with increases in total calorie intake (betas=0.25, 0.33; P<0.01). This may be due to wheat flour and rice intake: (a) being themselves, in terms of their own caloric content, main contributors to the total calorie intake; or (b) causing an increase in calorie intake from other sources. The former is more likely, given the effect below.
- The effect of total calorie intake on mortality from all cardiovascular diseases is insignificant when we control for the effects of rice and wheat flour intakes (beta=0.08; P=0.35). This suggests that neither wheat flour nor rice exerts an effect on mortality from all cardiovascular diseases by increasing total calorie intake from other food sources.
- Being female is significantly associated with a reduction in mortality from all cardiovascular diseases (beta=-0.24; P=0.01). This is to be expected. In other words, men are women with a few design flaws, so to speak. (This situation reverses itself a bit after menopause.)
Wheat flour displaces rice
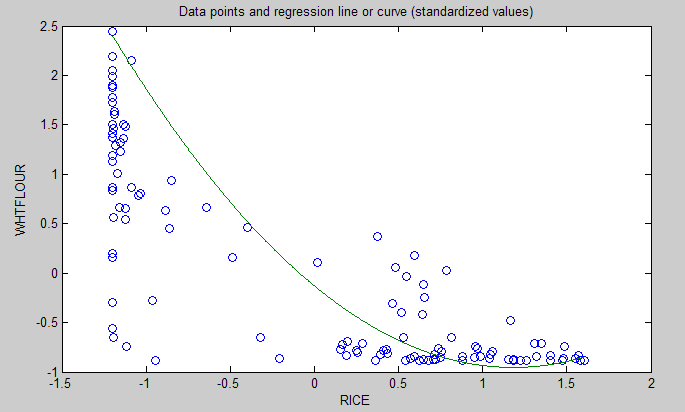
The graph below shows the shape of the association between wheat flour intake (WHTFLOUR) and rice intake (RICE). The values are provided in standardized format; e.g., 0 is the mean (a.k.a. average), 1 is one standard deviation above the mean, and so on. The curve is the best-fitting U curve obtained by the software. It actually has the shape of an exponential decay curve, which can be seen as a section of a U curve. This suggests that wheat flour consumption has strongly displaced rice consumption in several regions in China, and also that wherever rice consumption is high wheat flour consumption tends to be low.
As wheat flour intake goes up, so does cardiovascular disease mortality
The graphs below show the shapes of the association between wheat flour intake (WHTFLOUR) and mortality from all cardiovascular diseases (MVASC). In the first graph, the values are provided in standardized format; e.g., 0 is the mean (or average), 1 is one standard deviation above the mean, and so on. In the second graph, the values are provided in unstandardized format and organized in terciles (each of three equal intervals).


The curve in the first graph is the best-fitting U curve obtained by the software. It is a quasi-linear relationship. The higher the consumption of wheat flour in a county, the higher seems to be the mortality from all cardiovascular diseases. The second graph suggests that mortality in the third tercile, which represents a consumption of wheat flour of 501 to 751 g/day (a lot!), is 69 percent higher than mortality in the first tercile (0 to 251 g/day).
Rice seems to be protective, as long as intake is not too high
The graphs below show the shapes of the association between rice intake (RICE) and mortality from all cardiovascular diseases (MVASC). In the first graph, the values are provided in standardized format. In the second graph, the values are provided in unstandardized format and organized in terciles.


Here the relationship is more complex. The lowest mortality is clearly in the second tercile (206 to 412 g/day). There is a lot of variation in the first tercile, as suggested by the first graph with the U curve. (Remember, as rice intake goes down, wheat flour intake tends to go up.) The U curve here looks similar to the exponential decay curve shown earlier in the post, for the relationship between rice and wheat flour intake.
In fact, the shape of the association between rice intake and mortality from all cardiovascular diseases looks a bit like an “echo” of the shape of the relationship between rice and wheat flour intake. Here is what is creepy. This echo looks somewhat like the first curve (between rice and wheat flour intake), but with wheat flour intake replaced by “death” (i.e., mortality from all cardiovascular diseases).
What does this all mean?
- Wheat flour displacing rice does not look like a good thing. Wheat flour intake seems to have strongly displaced rice intake in the counties where it is heavily consumed. Generally speaking, that does not seem to have been a good thing. It looks like this is generally associated with increased mortality from all cardiovascular diseases.
- High glycemic index food consumption does not seem to be the problem here. Wheat flour and rice have very similar glycemic indices (but generally not glycemic loads; see below). Both lead to blood glucose and insulin spikes. Yet, rice consumption seems protective when it is not excessive. This is true in part (but not entirely) because it largely displaces wheat flour. Moreover, neither rice nor wheat flour consumption seems to be significantly associated with cardiovascular disease via an increase in total calorie consumption. This is a bit of a blow to the theory that high glycemic carbohydrates necessarily cause obesity, diabetes, and eventually cardiovascular disease.
- The problem with wheat flour is … hard to pinpoint, based on the results summarized here. Maybe it is the fact that it is an ultra-refined carbohydrate-rich food; less refined forms of wheat could be healthier. In fact, the glycemic loads of less refined carbohydrate-rich foods tend to be much lower than those of more refined ones (). (Also, boiled brown rice has a glycemic load that is about three times lower than that of whole wheat bread; whereas the glycemic indices are about the same.) Maybe the problem is wheat flour's gluten content. Maybe it is a combination of various factors (), including these.
Notes
- The path coefficients (indicated as beta coefficients) reflect the strength of the relationships; they are a bit like standard univariate (or Pearson) correlation coefficients, except that they take into consideration multivariate relationships (they control for competing effects on each variable). Whenever nonlinear relationships were modeled, the path coefficients were automatically corrected by the software to account for nonlinearity.
- The software used here identifies non-cyclical and mono-cyclical relationships such as logarithmic, exponential, and hyperbolic decay relationships. Once a relationship is identified, data values are corrected and coefficients calculated. This is not the same as log-transforming data prior to analysis, which is widely used but only works if the underlying relationship is logarithmic. Otherwise, log-transforming data may distort the relationship even more than assuming that it is linear, which is what is done by most statistical software tools.
- The R-squared values reflect the percentage of explained variance for certain variables; the higher they are, the better the model fit with the data. In complex and multi-factorial phenomena such as health-related phenomena, many would consider an R-squared of 0.20 as acceptable. Still, such an R-squared would mean that 80 percent of the variance for a particularly variable is unexplained by the data.
- The P values have been calculated using a nonparametric technique, a form of resampling called jackknifing, which does not require the assumption that the data is normally distributed to be met. This and other related techniques also tend to yield more reliable results for small samples, and samples with outliers (as long as the outliers are “good” data, and are not the result of measurement error).
- Only two data points per county were used (for males and females). This increased the sample size of the dataset without artificially reducing variance, which is desirable since the dataset is relatively small. This also allowed for the test of commonsense assumptions (e.g., the protective effects of being female), which is always a good idea in a complex analysis because violation of commonsense assumptions may suggest data collection or analysis error. On the other hand, it required the inclusion of a sex variable as a control variable in the analysis, which is no big deal.
- Since all the data was collected around the same time (late 1980s), this analysis assumes a somewhat static pattern of consumption of rice and wheat flour. In other words, let us assume that variations in consumption of a particular food do lead to variations in mortality. Still, that effect will typically take years to manifest itself. This is a major limitation of this dataset and any related analyses.
- Mortality from schistosomiasis infection (MSCHIST) does not confound the results presented here. Only counties where no deaths from schistosomiasis infection were reported have been included in this analysis. Mortality from all cardiovascular diseases (MVASC) was measured using the variable M059 ALLVASCc (ages 35-69).

33 comments:
Could this mean that a high-carb diet with no wheat is heart friendly? The japanese eat a lot of rice but almost no wheat.
I left a comment earlier but I guess it didn't take.
We'll give it another go. It seems that you results are indicating that blood sugar spikes aren't the issue.
Here we have to recognize that I don't put out a "health" blog but, for lack of a better term, a "sick" blog with a very limited focus.
All my info suggests that the rise in A1c and bad post prandials are a serious issue.
If I kept with your points, it seems that some aspect of wheat is doing damage (to beta cell functioning?)and what we're seeing is the consequence of that damage. I could take from this that wheat is like a battering ram that makes a breech in the system that allows things, that would not ordinarily be bad, to contribute to dysfunction with a definite downward trend.
You're making me crazy, Ned.
Hi Jason.
Yes, that is quite possible. We also have the Kitavans as another example.
Hi Michael.
The battering ram is a good analogy. That is one dataset only though.
We need to analyze other samples and populations as well.
Life is not that simple!
Recent analyses on this data are pretty revealing and bring up some interesting questions.
Foremost is how could the likes of Campbell and his group not see these things? In all critiques they seem to mainly fall back on the "uneducated" card. Should we then conclude they are educated and deliberate? If so, there are some evil implications here.
Wow, that's a lot of wheat!
I'll finish by saying this, when anyone I'm working with stops consuming wheat, they get better. All of them and no matter the disease or condition.
Great stuff. Did you develop WarpPLS?
Rice vs wheat is also a marker for climate and hence sun exposure since rice is characteristic of the traditional diets of those living in South China and Wheat of those living in the north. What we see here may have to do with sun exposure and Vitamin D not any demonic properties of wheat.
It is also possible that wheat is a marker for ethnic subgroups with different genetic makeups, or other socioeconomic factors. People eating wheat may be eating more trans fats for cultural reasons, for example.
Hi brian.
I try not to personalize data analyses. This post is a summary of what the data is telling us; not what anybody is telling us about the data.
Personalizing the discussion does generate some excitement, but is also distracting.
Yes, I developed WarpPLS. Currently working on version 2.0, plus other related projects.
The software has over 1,000 users worldwide, among them researchers at very prestigious research institutions around the world.
Still, it is good that this data is being analyzed by different people using different software tools. This reduces the probability of mistakes.
Hi Jenny.
Yes, good points.
On the vit D connection, wheat consump. doesn't seem to align well with North-South distribution. But the connection is worth looking into further.
The subpop.-specific adaptation idea is also one that needs to be looked into.
By the way, wheat flour is not yet demonized nearly to the same extent that cholesterol is. Certainly not like the "demon particle", the LDL.
I wonder if there are any studies of cured (non-wheat-consuming) celiacs that consider their cardiovascular or other health markers in comparison to their native population? If so, that would be another interesting piece of data to consider.
Scott W
Hi Scott.
Very good point. This study found that Scots who were "cured" celiacs did not have a higher chance of developing ischemic heart disease or stroke:
http://www.ncbi.nlm.nih.gov/pubmed/2744350
Does anybody know if there is anything in rice that could be cardio-protective?
This post by Don is not a real endorsement of rice, to say the least:
http://donmatesz.blogspot.com/2010/04/practically-paleo-perspective-rice.html
This study, apparently in Italy, found an association between celiac disease and autoimmune myocarditis:
http://circ.ahajournals.org/cgi/content/abstract/circulationaha;105/22/2611
Thanks Ned.
You can also try beige rice:
http://www.sciencenews.org/view/generic/id/58678/title/_This_off-white_rice_may_be_heart_healthy
I will never eat again any kind of rice/grains. Always ending in binges and no satisfy. Greetings.
Thanks Byron.
Interesting connection between rice and angiotensin by those folks at Temple and Wakayama.
I don't eat grains/seeds either. But it seems that, between rice and wheat, rice is a lot better.
"In other words, men are women with a few design flaws, so to speak."
Ha!
Thanks for doing this, Ned -- fascinating indeed.
One thing that may be obscuring the relationship between rice and heart disease is higher plasma folate, which tends to be higher in rice-eating regions due to higher intake of green veggies -- probably leading to lower homocysteine, even though it wasn't measured directly in the study.
Also, the rice-eating regions have a higher fish intake and much higher DHA status than elsewhere, which Campbell et al already analyzed and showed to be independently heart-protective in the data.
It may be interesting to integrate those things into a model and see if the behavior of rice changes.
Also, I'd suggest (if you get a chance) looking at the wheat and rice data from the questionnaire (the variables labeled "yearly ration of wheat" and "yearly ration of rice," I think. That wheat variable had a much stronger, nonlinear relationship with heart disease compared to the diet survey data. I'm not sure about rice.
Thanks Denise, very good points and suggestions, as always.
I haven't eaten wheat in years. I'm the healthiest person I know. After reading Denise's China Study analysis, I cut out grains, but with the seasonal change in weather I have begun craving rice. I feel better about giving in to those cravings now.
Hi,
Do the suggestion against eating wheat flour, apply equally to whole wheat?
What about Oat Bran?
Well, the data in this post is on wheat flour, and we cannot generalize the effects to whole wheat. But certainly wheat flour is much more refined than whole wheat, so I would expect the latter to be less harmful.
Still, grains and seeds are the plants' children, or children's reserves (so to speak). The plants absolutely don't "want" animals to eat them. Since plants cannot run or fight, they resort to other defenses, like toxins. This is why I generally avoid grains and seeds.
I assume you also avoid nuts, since they are also seeds?
Maybe I'm confusing my biology class (it's been a LONG time), but I thought plants want us to eat their fruits (and therefore disperse) their seeds.
There was an interesting program on pbs, called the Botany of Desire by Michael Pollan the other day, that basically talks about how plants have trained humans to do their bidding! (We generally think we are using plants.)
Hi Anon.
I do eat nuts, but not much. Nuts are a combination of fruit and seed. They are a bit different from seeds, and they also have another property: the shell is the plant's protection. That is, with nuts usually plants do not have to resort to toxins as a form of protection, since not many animals can break them.
Definitely plants evolved many mechanisms to make animals "do their bidding", primarily by dispersing their seeds through consumption of fruits. But one thing to bear in mind is that dead animals don't do those things, so it is reasonable to expect those mechanisms to be generally health-promoting.
Another important thing to bear in mind is that plants and animals co-evolved those mechanisms. That is, plants evolved certain mechanisms to entice animals to do certain things. But animals only do those things because they also evolved certain mechanisms; mechanisms that increased their reproductive success. For example, a plant may make a fruit very sweet, by turning it into a fructose bag. But if that leads to health deterioration over time, the animals that consume it will have decrease reproductive success. They will be over time replaced by animals with a different genotype.
Consider this. Since animals are attracted to sweetness, why don't we have plant species that produce fruits that are the equivalent to a chunk of table sugar? The reason is that they would not be favored by plant-animal co-evolution pressures.
Just wanted to add a comment I received from Dr. B.G. (from Animal Pharm) on possible confounders. She was answering an unrelated question, and referred to this post. Here it is:
"The cholesterol post was very illuminating and, though just epidemiological, appears to confirm outcomes from prospective trials like ERA and Framingham. FYI Chinese rural inhabitants probably cannot afford wheat as they do rice. Those consuming rice not wheat probably also had more sunlight, fresh air and more physical activity I'd suspect because they may be conceivably be working more outdoor manual labor type of activities."
Note that the comment above is unrelated to latitude, but to rural life. In counties that are more rural there may be more sunlight exposure, even if those counties are at higher latitudes.
Rural life is arguably healthier in terms of degenerative diseases, even though you may see higher mortality from infectious diseases in rural counties. This would have a double-effect in terms of confounding the results, if degree of "rurality" is strongly associated with rice consumption.
Spam comment above deleted.
I've read that in India it's the opposite: the rice eating south has far more heart disease than the wheat eaters in the north.
Hi Peter.
Thanks for the input. That is interesting. Do you happen to have a reference for that?
It is indeed possible that rice is simply a marker for something else in China that is healthy. That is, those who consume more rice may tend to exercise more, or spend more time outdoors.
Regarding India, I got this one, a study of samples from New Delhi (northern India) and Bangalore (southern India).
http://www.ajcn.org/cgi/content/abstract/79/4/582
The authors seem to believe that lower incidence of ischemic heart disease is due to the intake of vegetables and mustard oil. No mention of rice.
I eat a fair amount of seitan, which is basically just wheat gluten. Yes, the demon itself!
Seitan is very high-protein, very low-carb. (Like most things sourced from grains, relatively deficient in lysine, so it won't do as a primary protein source.)
I also have a number of friends who eat a lot of seitan. Over many years, none of us seem to have developed any of the problems for which gluten is so often blamed. That proves nothing, of course. We might all be lucky. Or we might be doing ourselves immense unseen damage.
Or, alternatively, it might be that gluten isn't really a problem when not accompanied by a flood of starch...
That is interesting David. It is possible that for those who are not gluten-intolerant, having it in a more isolate form than in bread and other wheat products could be healthier.
The isolation may reduce the amount of toxins naturally found in seeds, developed to fend-off seed predation by granivorous birds and other animals.
And, as you said, you don't get the highly refined carbs.
By the way, white rice is sometimes recommended over brown rice for the same reason (as in my comment above). That is, white rice may have lower amounts of the natural toxins in rice to prevent seed predation.
I think one of the cofounders here might be iron ... high iron levels in the blood are known to cause heart problems. Gluten causes at least temporary gut permeability, which as a "feel good" effect on a lot of people and hence people eat too much of it. But I think this gut permeability also allows too much iron into the bloodstream, esp. if the wheat flour in question happens to be enriched! And even more so if it is eaten with red meat (as it would be more in the non-fish-eating parts of China).
In India, turmeric is eaten a lot with meals, which blocks the iron, wheat or no wheat. And vegetarians who eat seitan are probably protected because the vegetarian diet is generally extremely low in iron (plus all those vegies block whatever iron might be in the meal).
High iron levels are also associated with impaired glucose handling, maybe because the glucose protects the body against the iron damage.
As for rice ... Chinese white rice isn't iron enriched I think, and brown rice is very good at blocking iron. However, in the US, white rice is often enriched with iron, so if the above theory pans out, eating American white rice would not have the same results as eating Chinese white rice!
I think we really have to take a hard look at iron absorption issues vs. heart disease and insulin. We worked so hard to get rid of anemia that I think we overdosed the population on iron.
Incidentally, people who are truly iron deficient often have celiac or parasites, both of which cause internal bleeding. Probably more of China is being treated for parasites these days, which might increase heart disease too.
hey nice info thnx for sharing this blog..
rice varieties
This post is a revised version of a previous post. The original comments are preserved here. More comments welcome, but no spam please!
Post a Comment